Reviewed by Brian St. Pierre, MS, RD and Helen Kollias, PhD
The debilitating experience of brain fog, memory lapses, and pervasive fatigue, often dismissed as typical signs of aging or misdiagnosed as depression, is increasingly being recognized as a central symptom of menopause, profoundly affecting millions of women globally. For many, like one woman in her late 40s, the descent into cognitive "sludge" began subtly but escalated into a life-altering challenge. What started as an inability to recall the name of a familiar restaurant – "Texas Roadhouse!" she’d later exclaim, hours after a frustrating conversation with her husband – soon manifested as a crippling inability to focus at work, a persistent haze that made even basic tasks feel insurmountable. This personal struggle, characterized by an unwelcome mental dullness, highlights a widespread issue: the often-overlooked neurological and psychological dimensions of the menopausal transition.
The Pervasive Enigma of Menopausal Brain Fog
The author’s journey began with what felt like a gradual erosion of her mental faculties. Simple recall, once effortless, became a monumental task. The names of friends, books, or movies would sit tantalizingly at the tip of her tongue, only to vanish into an inaccessible mental void. This "sludginess with proper nouns," while common in middle age, intensified to an alarming degree. Her professional life, which required sharp cognitive function and sustained concentration, suffered immensely. She describes staring at her computer screen, willing her fingertips to work, but feeling trapped in a perpetual state of "haze," akin to the groggy moments between sleep and full wakefulness. Productivity plummeted, and even leisure activities like reading became too demanding. On her worst days, the haze was insurmountable, rendering her incapable of work or engagement, feeling "barely alive."
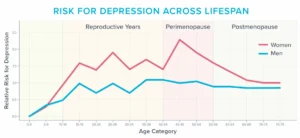
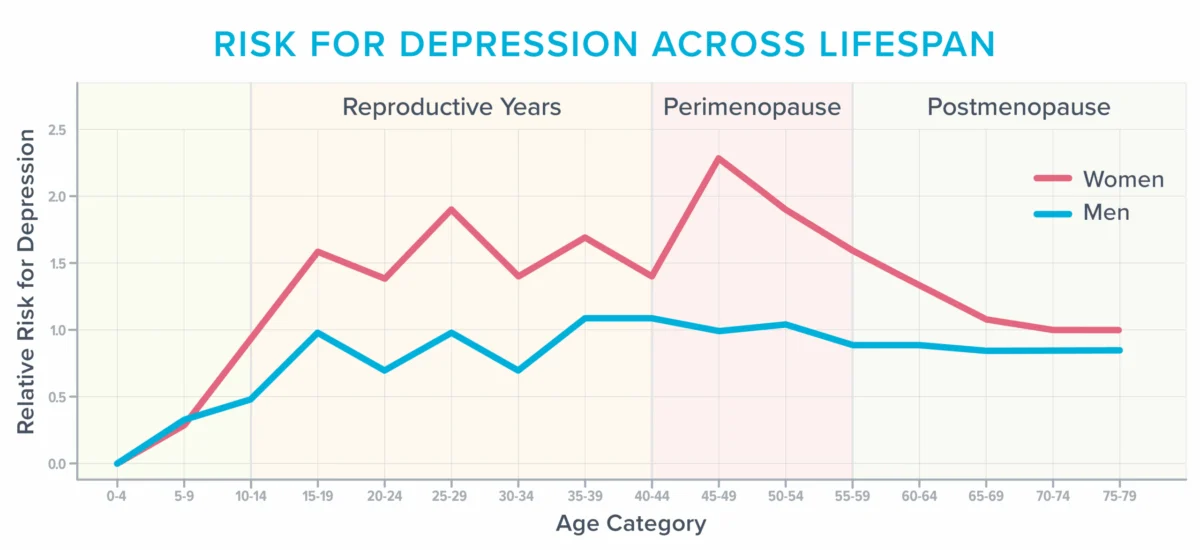
This experience is far from isolated. Millions of women navigating their late 40s and 50s report similar cognitive and emotional disturbances. The menopausal transition, defined as the period leading up to and including menopause (marked by 12 consecutive months without a menstrual period), is characterized by significant hormonal fluctuations. While symptoms like hot flashes and weight gain often receive primary attention, the impact on brain health and mental well-being is equally, if not more, profound for many. Studies indicate that approximately 40% of women experience increased irritability, mood swings, anxiety, fatigue, and difficulty concentrating during and after menopause, according to the American College of Obstetricians and Gynecologists. This percentage is likely conservative, as many women may not report these symptoms or connect them to menopause. Beyond individual suffering, the collective impact on workforce productivity and quality of life is substantial. This period also represents a heightened vulnerability for developing depression, particularly for those with a history of mood disorders, as evidenced by epidemiological data showing a distinct peak in depression risk for women around the perimenopausal years. The author’s personal account of inexplicable sobbing, heightened sensory sensitivity where normal sounds "literally hurt," and new anxieties underscores the severe emotional toll that often accompanies this profound biological shift.
A Challenging Diagnostic Landscape and the Path to Clarity
The path to understanding these symptoms is frequently fraught with misdirection. The author’s initial attempts to seek medical help illustrate a systemic challenge within healthcare. Over nearly two years, she consulted multiple professionals, receiving recommendations for various antidepressants. Each attempt left her feeling worse, turning her into a "zombie" with amplified drugged sensations from sleeping pills. Diagnostic tests for common culprits like thyroid dysfunction or anemia yielded no answers, further deepening her frustration and sense of helplessness. She resorted to an array of supplements, "mushroom coffee," and other purported brain-boosters, all to no avail, highlighting the desperation many women feel when conventional medicine offers no relief.
Her breakthrough came during a routine annual gynecological exam. A seemingly minor mention of vaginal dryness prompted her gynecologist to ask a series of comprehensive questions that, at first glance, seemed unrelated: "How was my sleep? Mood? Energy levels? Was I experiencing hot flashes? How about brain fog?" This holistic inquiry, which went beyond surface-level symptoms and connected seemingly disparate complaints, was the critical turning point. The connection between her various symptoms—vaginal dryness, fatigue, brain fog, and disturbed sleep—became clear. The diagnosis was not depression, but menopause. Within days of starting hormone therapy, specifically estradiol and progesterone, the fog lifted. Her cognitive function returned, sleep normalized, and she regained the capacity to work and engage with life. This rapid reversal underscored that her previous struggles were rooted in hormonal shifts, not a primary mental health disorder, offering a poignant example of the power of accurate diagnosis and targeted treatment.
Understanding Menopause: A Life Stage with Complex Health Implications
Menopause is not a disease but a natural biological stage in a woman’s life, marking the end of reproductive years. However, the profound hormonal changes, primarily the decline and fluctuation of estrogen, can trigger a cascade of symptoms affecting nearly every system in the body. While the physical symptoms are well-documented, the cognitive and emotional dimensions are often less understood by both patients and healthcare providers.

The underlying mechanisms driving these cognitive and emotional symptoms are multifaceted. Estrogen, a key hormone in this transition, plays a crucial role in regulating various brain functions. It influences the production and activity of neurotransmitters like serotonin, dopamine, and norepinephrine, which are vital for mood regulation, cognitive processing, and sleep architecture. Estrogen also impacts brain energy metabolism, neuroprotection, and cerebral blood flow. As estrogen levels fluctuate and decline during perimenopause and menopause, these critical brain functions can be disrupted. Compounding these hormonal shifts are typical age-related changes in the brain, which naturally occur as individuals age, such as a decrease in gray matter volume or changes in white matter integrity. Furthermore, this life stage often coincides with significant psychosocial stressors. Women in their 40s and 50s are frequently at the peak of their careers, shouldering immense professional responsibilities. Simultaneously, they may be navigating the complexities of parenting teenagers, caring for aging parents, adjusting to an empty nest, or facing financial pressures. Each of these factors can individually, and certainly collectively, siphon cognitive capacity and exacerbate feelings of overwhelm, mental fatigue, and emotional distress.
The Hidden Impact of Vasomotor Symptoms on Brain Health
Among the lesser-known, yet critically impactful, triggers for cognitive and emotional distress during menopause are vasomotor symptoms (VMS), commonly known as hot flashes and night sweats. These are more than mere inconveniences; mounting research suggests they have a direct and detrimental effect on cerebrovascular health and brain function.
During a hot flash or night sweat, the body undergoes a rapid physiological response. Norepinephrine and cortisol levels surge, leading to a dilation of blood vessels, increased heart rate, and elevated blood pressure as the body attempts to shed heat. These episodes can manifest with skin reddening, profuse sweating, heart palpitations, and feelings of anxiety, fatigue, or faintness. While the exact mechanism remains under investigation, one leading theory posits that falling estrogen levels disrupt the hypothalamus, the brain’s thermostat, causing it to misinterpret body temperature and trigger these intense heat-dissipation responses even when the body is not actually overheated.
For years, VMS were largely considered benign, albeit uncomfortable, symptoms. However, a growing body of evidence now indicates they may negatively impact blood vessels and the brain itself, leading many experts to reclassify VMS as a treatable medical condition requiring clinical attention.
Brain Lesions and Vascular Changes: A landmark study involving 226 women, utilizing monitors to track hot flashes and MRI scans to image their brains, revealed significant findings. Researchers observed an abundance of "whole-brain white matter intensities" – patchy lesions – in women who experienced the most frequent hot flashes. These lesions, once attributed solely to normal aging, are now understood by neuroscientists to be predictive of future cognitive decline. Individuals with a high prevalence of these brain lesions are twice as likely to be diagnosed with dementia and three times as likely to suffer a future stroke. This suggests a direct link between VMS severity and long-term cerebrovascular health risks, highlighting hot flashes as a potential early warning sign for future neurological issues.
Further research supports this vascular connection. A three-year study of 492 women found a correlation between frequent hot flashes and unhealthy changes in blood vessels, specifically a reduced ability of vessels to dilate and accommodate increased blood flow. Other research has linked frequent hot flashes with increases in arterial stiffness, endothelial dysfunction, and elevated C-reactive protein, all markers of systemic inflammation and cardiovascular disease risk. These vascular changes compromise brain blood supply, diminish the delivery of oxygen and nutrients, and increase the risk of microvascular damage, thereby contributing to cognitive impairment.
The Sleep-Brain Axis: Beyond direct vascular effects, frequent hot flashes profoundly disrupt sleep. Critically, many women are unaware that night sweats are the primary cause of their nocturnal awakenings. The surge of cortisol and norepinephrine can jolt them awake, but by the time they are conscious, the sensation of heat may have dissipated, leading them to believe they are simply experiencing insomnia or sleep apnea for no discernible reason. These repeated, often unrecognized, awakenings fragment sleep architecture, preventing the brain from entering crucial restorative phases of deep sleep and REM sleep. This fragmentation interferes with the brain’s ability to consolidate memories, metabolize metabolic toxins that accumulate during wakefulness (e.g., amyloid-beta, linked to Alzheimer’s), and properly store daily information. Chronic sleep deprivation also leads to reduced connectivity and volume in the hippocampus, a brain region essential for learning and memory. Furthermore, the amygdala, the brain’s emotional center, becomes hyper-reactive with insufficient sleep, contributing to increased stress, anxiety, irritability, frustration, and even rage. These adverse brain changes can manifest within days or weeks of insufficient sleep; imagine the cumulative impact over years of disturbed sleep during menopause.
Barriers to Effective Care: A Systemic Challenge
Despite the clear and significant