The experience of cognitive decline, often described as a "brain fog," affects a significant number of women in their late 40s and early 50s, frequently leading to misdiagnosis as depression. This critical period, known as perimenopause and menopause, marks a profound hormonal transition that can manifest in debilitating cognitive and emotional symptoms, profoundly impacting daily life and professional performance. The journey from confusion and misdiagnosis to understanding and effective treatment underscores a broader challenge within healthcare regarding menopause-specific education and awareness.
The Unseen Struggle: A Personal Account and Broader Prevalence
For many, the onset of menopausal brain fog is insidious, beginning with minor frustrations that escalate into pervasive cognitive impairment. One woman’s experience typifies this struggle: simple tasks like recalling a restaurant’s name became a frustrating ordeal, characterized by details "lost in a pile of sludge" only to resurface hours later. This difficulty with proper nouns, while common with aging, became alarmingly frequent and severe in her late 40s and early 50s. Beyond trivial memory lapses, her professional life suffered; staring at a computer screen, she would struggle to initiate work, her mind clouded by a persistent haze that often lasted the entire day. The fleeting moments of mental clarity, typically in the mornings, became a desperate race to condense eight hours of work into a mere two or three. On her worst days, the haze was insurmountable, rendering her unable to work, read, or engage in most activities.
This personal narrative is far from isolated. Research indicates that during and after menopause, approximately 40 percent of women report increased irritability, mood swings, anxiety, fatigue, and significant trouble concentrating. These symptoms are not merely inconveniences but represent a substantial degradation in quality of life and functional capacity. The period around perimenopause is also recognized as one of the most vulnerable times for women to develop depression, particularly for those with a prior history. This overlap in symptoms often leads to a diagnostic dilemma, where the underlying hormonal shifts of menopause are overlooked in favor of a depression diagnosis.
The Quest for Answers: A Medical Labyrinth
Faced with these profound changes, the search for medical help can be a protracted and disheartening journey. In the aforementioned case, a woman consulted three healthcare professionals, all of whom recommended antidepressants. Despite trying several different medications, including higher doses, her condition worsened, leaving her feeling "like a zombie" and "even more drugged." Other interventions, such as sleeping pills, proved equally ineffective. Comprehensive tests for thyroid issues and anemia yielded no abnormalities, further deepening the mystery of her deteriorating health. The pursuit of relief led her to various supplements, including "mushroom coffee" and products marketed for cognitive enhancement, none of which provided any lasting benefit.
It was only after nearly two years of this frustrating medical merry-go-round that a routine gynecological appointment provided a breakthrough. A casual mention of vaginal dryness, a common menopausal symptom, prompted her gynecologist to ask a series of questions that finally connected the dots: "How was my sleep? Mood? Energy levels? Was I experiencing hot flashes? How about brain fog?" The patient’s response, "Funny you should mention brain fog… I feel like I’m barely alive," unveiled the true nature of her affliction. She had not been battling depression, but rather the multifaceted symptoms of menopause. Prescriptions for estradiol and progesterone—forms of menopausal hormone therapy (MHT)—brought about a dramatic transformation within days. The fog lifted, cognitive function returned, sleep improved significantly, and the ability to work effectively beyond noon was restored.
Understanding Menopause: A Life Stage, Not a Disease
Menopause, fundamentally, is not a medical condition or a disease but a natural biological transition, akin to puberty. It signifies the permanent cessation of menstruation, diagnosed after 12 consecutive months without a period. The preceding phase, perimenopause, can last for several years, during which ovarian hormone levels—primarily estrogen and progesterone—fluctuate erratically before their eventual decline. These hormonal shifts trigger a wide array of symptoms, with weight gain and reduced sex drive often receiving considerable attention. However, the cognitive and emotional sequelae, though less frequently discussed, are equally impactful.
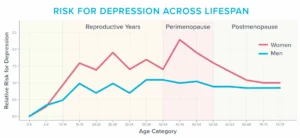
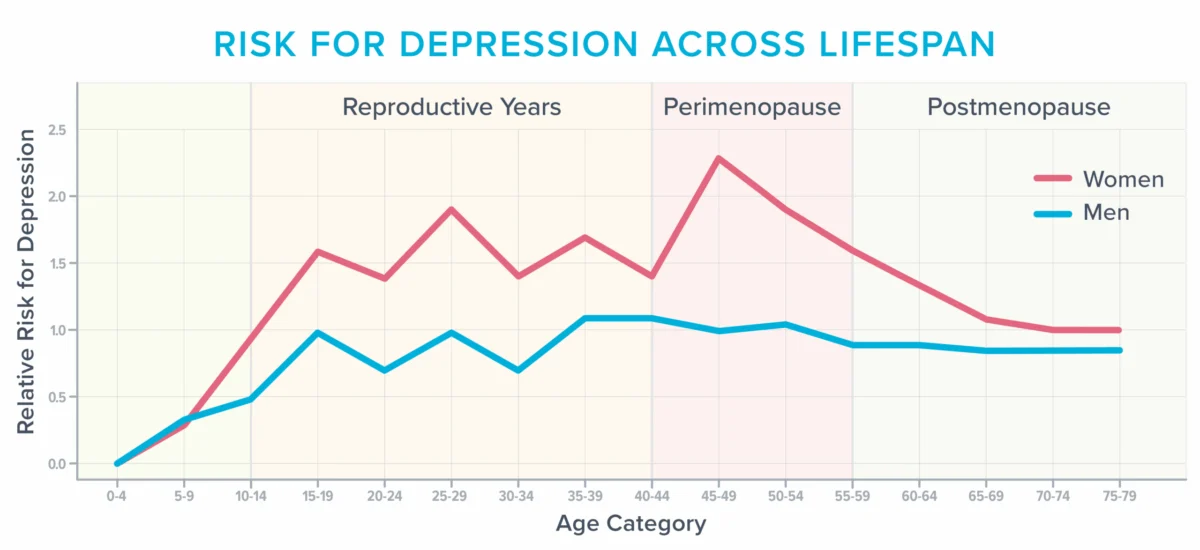
The graph illustrating the risk of depression across the lifespan highlights a critical point: while men’s risk remains relatively stable, women’s risk peaks significantly around the perimenopausal years, before gradually declining after age 50. This surge underscores the hormonal influence on mental health during this transitional period. Beyond the direct effects of fluctuating hormones, women in their 40s and 50s often face a convergence of life stressors—peak career responsibilities, parenting teenagers, caring for aging parents, or navigating significant life changes—all of which can exacerbate cognitive and emotional strain, further "siphoning cognitive capacity."
The Vexing Vasomotor Symptoms: Hot Flashes and Night Sweats
One of the most potent, yet often underappreciated, triggers for cognitive and emotional distress during menopause is the hot flash, and its nocturnal counterpart, night sweats. These are categorized as vasomotor symptoms (VMS), referring to the physiological processes involving the constriction and dilation of blood vessels. During a hot flash, there is a rapid surge in norepinephrine and cortisol, leading to blood vessel dilation, increased blood pressure, and elevated heart rate, all in an attempt to dissipate perceived excess heat. These episodes can manifest as skin reddening, sweating, heart palpitations, and sensations of anxiety, fatigue, or faintness.
For many years, VMS were largely considered mere inconveniences or sources of embarrassment. However, a growing body of research has revealed their profound systemic impact, extending beyond transient discomfort to affect blood vessels and brain health directly. Consequently, an increasing number of experts now advocate for considering VMS as a treatable medical condition. The exact mechanism of hot flashes is not fully understood, but one prominent theory implicates falling estrogen levels in disrupting the hypothalamus, the brain’s thermoregulatory center, leading to a "wonky" internal thermostat that misinterprets body temperature.
Vasomotor Symptoms and Brain Health: A Deeper Look
Emerging research has shed light on how frequent VMS can induce measurable changes in the brain, potentially predisposing women to future cognitive decline. A study involving 226 women, utilizing monitors to track hot flashes, MRI scans, sleep diaries, and smartwatches, found a significant correlation. Women who experienced the most frequent hot flashes exhibited an abundance of "whole-brain white matter intensities" on their MRI scans. These patchy areas, once thought to be benign age-related changes, are now considered predictive of future cognitive decline. Individuals with a high prevalence of these brain lesions face double the risk of developing dementia and triple the risk of future stroke, highlighting the serious implications of untreated VMS.
The link between hot flashes and these brain lesions is thought to originate from their impact on the brain’s delicate vascular system. A three-year study of 492 women supported this theory, demonstrating that frequent hot flashes were associated with unhealthy changes in blood vessel function, specifically a reduced ability to dilate in response to increased blood flow. Other research has further linked frequent hot flashes to increased arterial stiffness, carotid intima-media thickness (an indicator of atherosclerosis), and levels of C-reactive protein (a marker of systemic inflammation), all of which contribute to cardiovascular risk and, by extension, brain health.

The Critical Sleep-Brain Connection
Beyond direct vascular effects, frequent hot flashes significantly disrupt sleep, which in turn exacerbates cognitive and emotional symptoms. Many women experiencing night sweats may not even recognize them as the cause of their disturbed sleep, often attributing their awakenings to general insomnia or sleep apnea. This is because the intense heat of a night sweat can dissipate by the time the surge of cortisol and norepinephrine jolts them awake, leaving them to wonder why they are repeatedly waking "for no discernable reason."
These frequent nocturnal awakenings have serious repercussions for brain function. They impede the brain’s ability to consolidate memories, metabolize toxins accumulated during waking hours, and process daily information. Chronic sleep disruption can also lead to reduced connectivity in the hippocampus, a brain region vital for learning and memory. Furthermore, sleep loss renders the amygdala, the brain’s emotional center, more reactive, leading to heightened stress, anxiety, irritability, frustration, and even rage. These adverse brain changes can manifest within days to a week of insufficient sleep, making the cumulative impact of years of disrupted sleep due to VMS profoundly detrimental.
Navigating the Medical Labyrinth: Challenges in Diagnosis and Treatment
The path to appropriate care for menopausal symptoms is often fraught with obstacles. One significant challenge lies in the overlap of symptoms between menopause-related sleep deprivation and clinical depression. Diagnostic tools like the Patient Health Questionnaire (PHQ-9) depression scale include symptoms such as trouble sleeping, feeling tired or having little energy, changes in appetite, and difficulty concentrating—all of which are common in perimenopause and menopause. Checking off just four of these nine symptoms can lead to a depression diagnosis, potentially diverting attention from the underlying hormonal cause.
A critical systemic issue is the widespread lack of menopause-specific training among healthcare professionals. Surveys reveal that 80 percent of medical residents feel "barely comfortable" discussing menopause, and few residency programs, even in obstetrics and gynecology, offer comprehensive training in this area. This educational deficit explains why many professionals fail to inquire about hot flashes or sleep disturbances when women present with fatigue, lack of motivation, and cognitive difficulties.
Even when VMS are clearly identified as contributing to cognitive and emotional symptoms, many healthcare professionals remain hesitant to prescribe menopausal hormone therapy (MHT), often citing concerns about safety and risk. This reluctance, according to Michigan-based menopause-trained gynecologist Dr. Jerrold H. Weinberg, often stems from "defensive medicine," a practice driven by fear of malpractice lawsuits.
Revisiting Menopausal Hormone Therapy (MHT): Debunking Myths and Modern Understanding
The apprehension surrounding MHT largely originates from research conducted decades ago, particularly the Women’s Health Initiative (WHI) study, which linked certain types of hormones to a slightly increased risk of breast cancer and stroke. However, more recent and nuanced research has refined this understanding. It indicates that the small increased risks are highly dependent on factors such as a woman’s age, the specific dose and type of hormonal preparation, and the duration of hormone use.
Current consensus among many experts suggests that for women under 60 and fewer than 10 years postmenopausal, particularly those with moderate to severe menopausal symptoms, the benefits of MHT often outweigh the risks. Dr. Weinberg emphasizes that MHT offers substantial health benefits, including a reduced risk of developing Alzheimer’s disease and osteoporosis. He asserts that for most women, these benefits far surpass the potential risks when prescribed appropriately. While some antidepressants can alleviate mood disturbances, improve sleep, and even reduce hot flashes, they come with their own side effect profiles and, for a clinician practicing defensive medicine, may appear as a "safer bet" than MHT. However, for those suffering from true menopausal symptoms, MHT often provides a more direct and effective solution by addressing the root hormonal imbalance.
Empowering Advocacy: Strategies for Seeking Effective Care
Given the complexities of diagnosis and treatment, women experiencing menopausal symptoms must become proactive advocates for their own health. Dr. Weinberg and Helen Kollias, PhD, a physiology and molecular biology expert and science advisor at Precision Nutrition and Girls Gone Strong, offer practical advice:
- Seek Menopause-Trained Professionals: Prioritize healthcare providers who specifically list menopause as an area of focus or hold certifications from reputable organizations like the Menopause Society (formerly NAMS). Online databases can help locate such practitioners.
- Document Symptoms Meticulously: Keep a detailed record of symptoms, including their frequency, severity, and impact on daily life. This documentation serves as a reliable reference during appointments, especially if brain fog or anxiety makes it difficult to recall details. Track hot flashes (number, severity), sleep quality (hours, awakenings), mood fluctuations, energy levels, and cognitive function.
- Be Specific in Communication: Vague statements like "I don’t sleep well" are less effective than precise descriptions, such as "During the past seven days, I’ve only had four uninterrupted hours of sleep once, waking an average of five times a night, with my longest stretch being three hours." Utilize data from smartwatches or health apps to provide objective metrics.
- Engage in Shared Decision-Making: Actively participate in discussions about treatment options, including their benefits and risks. This collaborative approach, encouraged by many healthcare networks, empowers patients and can help clinicians move beyond a "defensive medicine" mindset. Ask specific questions: "What are the benefits of this treatment for my specific symptoms?" "What are the risks?" "What are the alternatives?" "What happens if I choose not to treat?"
Holistic Approaches: Lifestyle Interventions for Menopausal Well-being
Beyond medical interventions, lifestyle strategies play a crucial role in managing menopausal symptoms and improving overall mental and emotional health. While there’s no "special diet" beyond avoiding known triggers like caffeine, alcohol, and spicy foods (and soy products have shown limited efficacy for VMS), fundamental health habits remain paramount.
- Lean into Fundamental Health Strategies: Re-evaluate and prioritize core health behaviors. Ensure adequate nutrient intake, regular physical activity, effective stress management, sufficient sleep, strong social connections, and a sense of purpose. Middle age often demands a recalibration of these fundamentals.
- Experiment with Creatine: This supplement, known for its role in muscle and bone health, may also boost mood and brain function, reduce mental fatigue, and counteract some negative effects of sleep deprivation. A daily dose of 5-7 grams of creatine monohydrate is typically recommended.
- Get Regular Light Exposure: Morning and late afternoon sunlight exposure helps regulate the body’s circadian rhythm, promoting alertness during the day and better sleep at night. Studies show that morning outdoor light exposure leads to faster sleep onset, longer sleep duration, and fewer awakenings. Sunlight also positively impacts mood and concentration.
- Go Easier at the Gym: Intense, prolonged exercise can be counterproductive during menopause, increasing injury risk and recovery time, and exacerbating irritability and fatigue. Instead, incorporate short bursts of moderate activity, like a 5-10 minute walk or a quick set of squats, to boost alertness. Gentle exercises like yoga or stretching can aid relaxation before bed, but avoid intense workouts close to bedtime to prevent adrenaline release. Listen to your body, adjusting intensity and volume based on sleep and recovery.
- Investigate Cognitive Behavioral Therapy for Insomnia (CBT-I): This evidence-based therapy equips individuals with skills and cognitive reframes to improve sleep quality. Techniques include maintaining a consistent wake-up time, regardless of prior night’s sleep, and addressing sleep-related anxieties.
- Get Real About Stress: Menopause often coincides with peak life demands. Critically assess responsibilities and bandwidth. Track time and energy expenditure to identify areas for reduction or delegation. Questions to consider include: "What can I let go of?" "What can I simplify?" "Where can I ask for help?" The "Wheel of Stress Assessment" can help identify specific stressors. Learning to say "no" more often can significantly free up mental and emotional capacity.
- Experiment with Cooling Technology: A cooler sleep environment can reduce night sweats and improve sleep quality. Options include lowering the thermostat, using fans, or investing in electric cooling mattress pads.
- Take Frequent Breaks: When brain fog sets in, productivity plummets. Permit short periods of inactivity, such as a 20-minute rest, mindful breathing, or a brief walk. A 5-minute mind-body scan can also offer a quick "refresh," allowing for non-judgmental observation of physical sensations and thoughts, leading to a clearer sense of needs.
- Follow a Diet that Promotes Healthy Circulation: A diet rich in vegetables, fruits, whole grains, healthy fats (like olive oil), beans, and fish, mirroring the MIND and Mediterranean diets, is associated with a reduced risk of Alzheimer’s disease and depression. Nitrate-rich foods such as beets and dark leafy greens can temporarily improve memory by promoting blood vessel dilation and increasing blood flow to the brain.
The Upside of Menopause: An Opportunity for Reassessment and Growth
While the challenges of menopausal symptoms can be profoundly frustrating, this life stage also presents a unique opportunity for introspection and re-evaluation. The diminishing capacity to "do it all" can force a critical assessment of priorities. For the individual whose story opened this discussion, the struggle to produce coherent work prompted an existential question: "Do I really need to be doing this?" This inquiry allowed her to reassess how to allocate her finite mental resources. Recognizing the privilege of self-employment, she no longer felt compelled to work eight hours a day. Similarly, domestic responsibilities were simplified, and the power of saying "no" became a tool to preserve energy for what truly mattered: family connections, meaningful friendships, and personal well-being.
With the aid of hormone therapy and intentional lifestyle adjustments, energy and mental clarity returned. Yet, the choice to conclude her workday earlier persists, not out of necessity, but out of a newfound appreciation for prioritizing personal time. Menopause, therefore, can be reframed not just as a period of challenges, but as a transformative phase that encourages women to redefine success, embrace self-care, and cultivate a life aligned with their deepest values and evolving needs.