For many women navigating their late 40s and early 50s, the experience of cognitive decline and profound emotional shifts can be bewildering, often mistaken for other conditions like depression. What begins as a frustrating inability to recall proper nouns, like the name of a familiar restaurant with peanut shells on the floor – “Texas Roadhouse!” – can escalate into a pervasive mental fog, significantly impacting daily function and professional life. This personal struggle, described as having "thoughts under a pile of garbage," reflects a widespread, yet frequently misdiagnosed, challenge faced by millions: the intricate and often debilitating effects of menopause on the brain.
The Pervasive Fog: A Common, Yet Misunderstood, Experience
The onset of perimenopause and menopause can usher in a cascade of symptoms far beyond the well-known hot flashes and night sweats. For the individual experiencing it, the shift can be profound. Tasks that were once routine, like focusing on a computer screen for an eight-hour workday, become monumental hurdles. The brain’s capacity, once reliable, seems to diminish, leaving a lingering haze that makes even basic cognitive functions feel like slogging through mud. Mornings might offer a brief window of clarity, but for many, particularly on the worst days, this mental dullness persists, rendering productive work, reading, or even simple engagement impossible. This significant drop in cognitive function, including impaired concentration, memory lapses, and reduced mental stamina, is a hallmark of what is increasingly recognized as menopause-related brain fog.
A Diagnostic Labyrinth: The Journey to Understanding
The path to diagnosis for these complex symptoms is frequently fraught with misdirection. The individual in question recounts a nearly two-year odyssey through various healthcare professionals, each offering solutions that missed the mark. Antidepressants, tried in different forms and dosages, only exacerbated feelings of lethargy and detachment, akin to becoming a "zombie." Sleeping pills left her feeling further drugged. Routine tests for thyroid issues or anemia came back normal, ruling out common physical causes. This protracted search highlights a critical gap in medical understanding and training regarding menopause. The turning point arrived during a routine gynecological exam, when a casual mention of vaginal dryness prompted a series of questions about sleep, mood, energy levels, hot flashes, and, crucially, brain fog. It was then, in a hazy monotone, that the patient uttered, "I feel like I’m barely alive," finally leading to the revelation that her struggles were not depression, but menopause.
Menopause: A Life Stage with Profound Systemic Impact
Menopause is not a disease or a medical condition but a natural biological transition, marking the end of a woman’s reproductive years. It is officially declared after 12 consecutive months without a menstrual period. The period leading up to this, known as perimenopause, can last for several years, during which ovarian hormone production, primarily estrogen and progesterone, fluctuates wildly before ultimately declining. These hormonal shifts are responsible for the wide array of symptoms experienced by women. While symptoms like weight gain and reduced libido often garner significant attention, the cognitive and emotional impacts are equally, if not more, prevalent and disruptive.
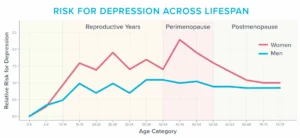
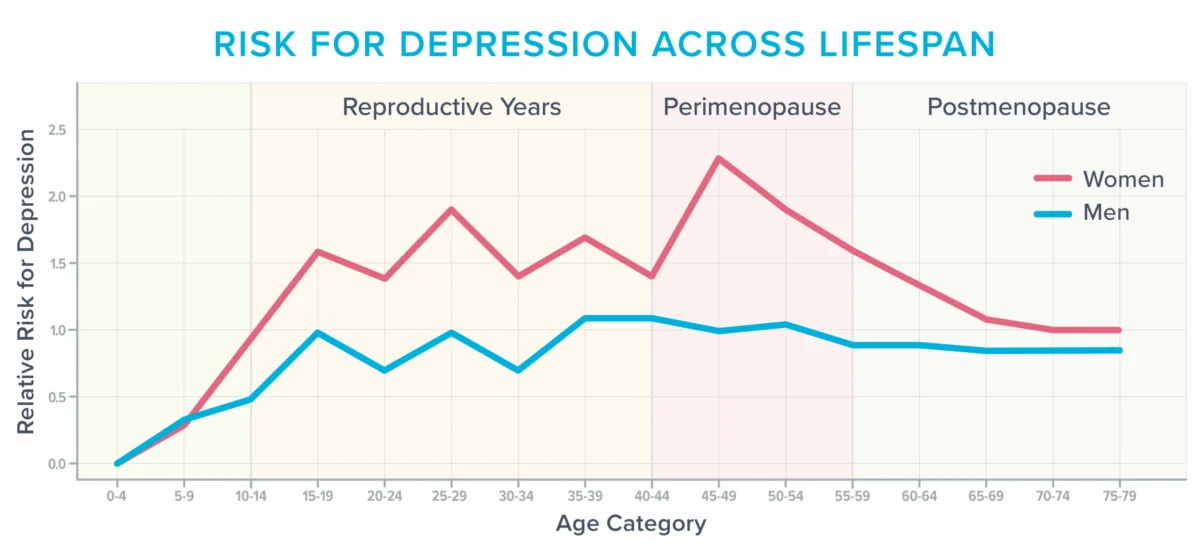
According to the American College of Obstetricians and Gynecologists (ACOG), approximately 40% of women report increased irritability, mood swings, anxiety, fatigue, and difficulty concentrating during and after menopause. Data from various studies consistently show that women’s risk of developing depression peaks around the perimenopausal years, particularly for those with a history of mood disorders. This makes the menopausal transition one of the most vulnerable periods for mental health challenges. The fluctuations in estrogen, a hormone with widespread influence on brain function, neurotransmitter regulation, and blood flow, are central to these changes. Estrogen receptors are abundant in brain regions critical for mood, memory, and executive function, such as the hippocampus, amygdala, and prefrontal cortex. As estrogen levels decline, these brain areas can be significantly affected, contributing to symptoms like anxiety, heightened sensory sensitivity (e.g., normal sounds causing physical pain), and a general sense of unease or panic in previously unbothered situations.
Beyond Hormones: The Multi-faceted Contributors to Menopausal Brain Fog
While hormonal shifts are a primary driver, the cognitive and emotional symptoms of menopause are often a complex interplay of physiological changes and significant life stressors. During their 40s and 50s, many women are at the zenith of their careers, shouldering immense professional responsibilities. Simultaneously, they may be navigating the complexities of parenting teenagers, caring for aging parents, adjusting to an empty nest, or facing significant financial pressures from college tuition or healthcare costs. These multifarious demands place an enormous strain on cognitive reserves, potentially siphoning mental capacity faster than the body can replenish it.
However, a lesser-known, yet critically important, factor contributing to cognitive distress is the hallmark menopausal symptom itself: vasomotor symptoms (VMS), commonly known as hot flashes and night sweats. These seemingly simple inconveniences are now understood to have profound implications for brain health.
The Anatomy and Impact of Vasomotor Symptoms (VMS)
Vasomotor symptoms involve the constriction and dilation of blood vessels, influencing blood pressure, heart rate, and sweating. During a hot flash or night sweat, there’s a surge in norepinephrine and cortisol, leading to rapid blood vessel dilation, skin reddening, and a sensation of intense warmth spreading across the face, neck, and chest. Heart palpitations, anxiety, fatigue, and even faintness can accompany these episodes. While the exact mechanism remains under investigation, one leading theory suggests that falling estrogen levels disrupt the hypothalamus, the brain’s temperature-regulating center, causing it to misinterpret normal body temperature as excessively hot or cold.
For years, VMS were largely dismissed as mere annoyances. However, a growing body of research has unveiled their deeper, more insidious effects on the brain and cardiovascular system. Increasingly, experts are recognizing VMS as a treatable medical condition, not just a transient discomfort. Studies utilizing objective measures like skin conductance monitors to track hot flashes, combined with magnetic resonance imaging (MRI) of the brain, have provided compelling evidence. One notable study involving 226 women revealed that those experiencing the most frequent hot flashes exhibited a higher abundance of "whole-brain white matter intensities" – patchy areas in the brain that neuroscientists now link to future cognitive decline, increased risk of dementia, and stroke.
The connection appears to stem from the impact of VMS on the brain’s delicate vascular network. A three-year study of 492 women demonstrated that frequent hot flashes correlated with unhealthy changes in blood vessels, specifically a reduced ability to dilate and accommodate increased blood flow. This vascular compromise can impair the delivery of oxygen and nutrients to brain tissue. Furthermore, frequent hot flashes have been linked to increased oxidative stress, inflammation, blood-brain barrier permeability, and even a reduction in brain-derived neurotrophic factor (BDNF), a protein crucial for neuron growth and survival.
The Critical Role of Sleep Disruption
Beyond direct vascular effects, VMS severely disrupt sleep, which has cascading negative consequences for brain health. Many women may not consciously attribute their sleep disturbances to night sweats, often assuming they have insomnia or sleep apnea. This is because the immediate "hotness" of a night sweat might dissipate by the time a woman is jolted awake by the surge of cortisol and norepinephrine. Consequently, she experiences repeated, seemingly unprovoked awakenings throughout the night.

Chronic sleep deprivation, even partial, profoundly impacts cognitive function. It impairs the brain’s ability to consolidate memories, process daily information, and efficiently clear metabolic waste products and toxins. Research shows that just days to a week of insufficient sleep can lead to reduced connectivity in the hippocampus, a brain region vital for learning and memory. Moreover, sleep loss increases the reactivity of the amygdala, the brain’s emotional center, making individuals more prone to stress, anxiety, irritability, and anger. Imagine the cumulative effect of years of such fragmented sleep. This chronic disruption directly contributes to the brain fog, memory issues, and emotional dysregulation frequently reported during menopause.
The Systemic Challenge: Misdiagnosis and Treatment Barriers
The widespread misdiagnosis of menopause-related cognitive and emotional symptoms stems from several systemic issues within healthcare. Diagnostic tools like the Patient Health Questionnaire (PHQ-9) depression scale, commonly used to screen for depression, contain several symptom overlaps with menopause-related sleep deprivation. For instance, questions about trouble sleeping, fatigue, changes in appetite, and difficulty concentrating can all be symptoms of menopausal sleep disturbance rather than primary depression. Checking off four such items can lead to a depression diagnosis, diverting attention from the underlying hormonal cause.
A significant contributing factor is the alarming lack of menopause-specific training in medical education. Surveys indicate that up to 80% of medical residents feel "barely comfortable" discussing menopause, and few residency programs, including OB/GYN, offer comprehensive training in this area. This educational deficit means healthcare professionals often fail to inquire about hot flashes or sleep disturbances when women present with fatigue, lack of motivation, and concentration issues.
Furthermore, even when VMS are identified as contributors to cognitive and emotional symptoms, many healthcare professionals remain hesitant to prescribe menopausal hormone therapy (MHT), also known as hormone replacement therapy (HRT). This reluctance often stems from what Dr. Jerrold H. Weinberg, a menopause-trained gynecologist, describes as "defensive medicine," driven by concerns about litigation and past controversies.
Revisiting Menopausal Hormone Therapy (MHT): A Nuanced Perspective
The apprehension surrounding MHT largely originates from the Women’s Health Initiative (WHI) study, published in the early 2000s. This landmark study, which involved hundreds of thousands of women, initially suggested an increased risk of breast cancer, heart disease, and stroke with hormone therapy. The findings led to a dramatic decline in MHT prescriptions and a generation of physicians cautious about its use.
However, subsequent re-analyses and more recent research have provided a significantly more nuanced understanding. It is now widely accepted that the risks and benefits of MHT are highly dependent on several factors, including the woman’s age, the specific type of hormonal preparation (e.g., estrogen-only versus estrogen-progestin), the dose, and the duration of use. Current guidelines from major medical organizations, such as ACOG and the Menopause Society (formerly NAMS), state that for women younger than 60 and within 10 years of their last menstrual period, the benefits of MHT often outweigh the risks, particularly for those experiencing moderate to severe menopausal symptoms.
These benefits extend beyond symptom relief, potentially including a reduced risk of osteoporosis and, for some, a protective effect against Alzheimer’s disease. Dr. Weinberg emphasizes that for most women in the appropriate age window, the overall health benefits often surpass the potential risks. While antidepressants can offer some relief for mood symptoms and even reduce hot flashes, they come with their own side effect profiles and do not address the underlying hormonal deficiency or provide the bone and cognitive benefits associated with MHT. For a clinician practicing defensive medicine, however, antidepressants might still appear as a "safer" option, despite not being a targeted treatment for menopause.
Empowering Advocacy: Navigating Menopausal Healthcare
Given the complexities, women must become proactive advocates for their health during menopause. Experts like Dr. Weinberg and Helen Kollias, PhD, a science advisor at Precision Nutrition, offer critical advice:
- Seek Menopause-Trained Professionals: Prioritize healthcare providers who explicitly list menopause as a focus area or hold certifications from reputable organizations like the Menopause Society. Specialized knowledge is key to accurate diagnosis and appropriate treatment.
- Document Symptoms Meticulously: Maintain a detailed log of symptoms, including their nature, severity, frequency, and any potential triggers. This provides concrete data for appointments, especially when brain fog might make recall difficult. Track sleep patterns (duration, awakenings), hot flashes (time, intensity), mood fluctuations, energy levels, and cognitive complaints.
- Be Specific in Communication: Vague statements like "I don’t sleep well" are less effective than precise descriptions, such as "During the past seven nights, I’ve had only one uninterrupted four-hour stretch of sleep, waking an average of five times per night." Utilize data from smartwatches or sleep trackers to provide objective evidence.
- Engage in Shared Decision-Making: Actively participate in treatment discussions. Ask about the specific benefits and risks of all proposed treatments, including MHT, tailored to your individual health profile. Inquire about alternative therapies, potential side effects, and monitoring protocols. This collaborative approach can help shift a clinician away from a defensive stance and ensure your preferences are considered.
Holistic Strategies for Enhancing Mental and Emotional Health
While medical intervention can be transformative, a comprehensive approach to menopausal well-being also heavily relies on lifestyle strategies. Beyond avoiding common triggers like caffeine, alcohol, and spicy foods, there isn’t a single "menopause diet," but general healthy eating patterns are crucial.
- Reinforce Fundamental Health Habits: Core behaviors like balanced nutrition, regular physical activity, stress management, adequate sleep, social connection, and a sense of purpose become even more critical. Regularly assess if these fundamentals are being met and identify barriers to their implementation.
- Experiment with Creatine: This supplement, known for muscle and bone health, also shows promise in bolstering mood, brain function, and reducing mental fatigue, potentially counteracting some negative effects of sleep deprivation. A daily dose of 5-7 grams of creatine monohydrate is often recommended.
- Optimize Light Exposure: Regular exposure to natural light, especially in the morning and late afternoon, helps regulate the body’s circadian rhythm, promoting alertness during the day and better sleep at night. Sunlight also has documented benefits for mood and concentration.
- Mindful Exercise Adjustments: While exercise remains vital, intense, long sessions can exacerbate fatigue and irritability, especially with compromised recovery. Short bursts of movement (e.g., a 10-minute walk) can boost alertness. Gentle activities like yoga can aid relaxation before bed. Listen to your body, adjusting intensity and volume based on sleep quality and recovery, opting for moderate sessions or reducing sets/reps when needed.
- Explore Cognitive Behavioral Therapy for Insomnia (CBT-I): This evidence-based therapy equips individuals with skills and mental reframes to improve sleep quality, such as maintaining a consistent wake-up time regardless of prior night’s sleep.
- Realistically Manage Stress: Critically evaluate responsibilities and commitments. Track time and bandwidth to identify drains on mental and emotional capacity. Prioritize, delegate, or eliminate tasks that are not essential. Learning to say "no" more often can free up vital resources for self-care.
- Utilize Cooling Technologies: A cooler sleep environment can reduce night sweats and improve sleep quality. This can involve adjusting thermostats, using fans, or investing in cooling mattress pads.
- Implement Frequent Breaks: When brain fog descends, productivity wanes. Permit short breaks (20 minutes) for relaxation: gazing out a window, listening to music, light stretching, or a brief mind-body scan to observe physical and mental sensations without judgment.
- Adopt a Circulation-Promoting Diet: Diets like the Mediterranean and MIND diets, rich in vegetables, fruits, whole grains, lean proteins, and healthy fats, support cardiovascular health, including the blood vessels in the brain. Nitrate-rich foods like beets and leafy greens may temporarily enhance memory by improving cerebral blood flow.
The Broader Implications and a Call for Re-evaluation
The misdiagnosis and undertreatment of menopause-related cognitive and emotional symptoms represent a significant public health challenge. Beyond individual suffering, there are broader societal and economic implications, including lost productivity, increased healthcare costs from inappropriate treatments, and a diminished quality of life for a substantial portion of the female population.
Yet, this challenging life stage also presents a unique opportunity for re-evaluation and empowerment. As cognitive resources become more limited, women are often compelled to scrutinize their priorities, asking fundamental questions about what truly matters. For the individual whose journey inspired this discussion, her diminished capacity forced a re-assessment of work hours, domestic responsibilities, and social commitments. This led to simplifying life, prioritizing essential relationships, and intentionally carving out time for personal well-being. The "gift" of forced re-evaluation ultimately resulted in a more intentional and fulfilling life, even after hormonal balance was restored.
By shedding light on the intricate connection between menopause and brain health, promoting better medical education, and empowering women to advocate for themselves, society can move towards a future where this natural transition is understood, appropriately managed, and even embraced as a period of profound self-discovery and realignment.