The experience of a professional writer struggling to recall basic facts, staring blankly at a computer screen, and feeling an inexplicable mental haze is a narrative far too common among women navigating the perimenopausal and menopausal transitions. What often manifests as debilitating brain fog, memory lapses, and profound fatigue is frequently misdiagnosed as depression, leading to years of ineffective treatments and profound frustration. This article delves into the personal account of such a journey, the scientific underpinnings of menopause-related cognitive and emotional symptoms, and the systemic challenges women face in receiving appropriate care, alongside actionable strategies for health advocacy and lifestyle management.
A Personal Battle Against the Fog
The initial signs were subtle, yet increasingly pervasive: a simple dinner decision turning into a frustrating attempt to recall a restaurant’s name, its location, or even distinct features like "peanut shells on the floor." What began as typical age-related difficulty with proper nouns in one’s late 40s soon escalated into a profound cognitive impairment. The individual described her thoughts as being "under a pile of garbage," her brain "pooping out during the workday," and waking with a haze that made work a "non-starter." This wasn’t merely forgetfulness; it was a pervasive mental sluggishness that impacted concentration, productivity, and overall quality of life. The mental clarity, once a constant, became a fleeting visitor, usually confined to the early morning hours, forcing an eight-hour workday into a mere two or three.
The emotional toll was equally significant. Beyond the cognitive struggles, the individual experienced unexplained bouts of crying, heightened sensitivity to everyday sounds like traffic or mall chatter, describing them as physically painful. Jumpy, irritable, and anxious about previously mundane situations like driving over bridges, she felt "barely alive." This constellation of symptoms, unfortunately, led to a familiar diagnostic path.
The Peril of Misdiagnosis: A Systemic Issue
Seeking medical advice, the individual encountered a revolving door of healthcare professionals. Three recommended antidepressants, each tried with worsening side effects, leaving her feeling like a "zombie." A sleeping pill only exacerbated the drugged sensation. Extensive tests for thyroid issues and anemia yielded no answers. Desperate, she experimented with supplements, mushroom coffee, and any product promising to boost brain function. This two-year odyssey highlights a critical gap in women’s healthcare: the frequent failure to connect these symptoms to the perimenopausal or menopausal transition.
It was only during a routine annual gynecological exam, prompted by a seemingly unrelated complaint of vaginal dryness, that a physician finally connected the dots. The gynecologist’s subsequent questions—about sleep, mood, energy levels, hot flashes, and brain fog—unlocked the true diagnosis: menopause. The prescribed estrogen (estradiol) and progesterone brought almost immediate relief, akin to "someone had flipped a switch." Within days, cognitive function returned, sleep improved dramatically, and the pervasive haze lifted. This anecdotal account mirrors the experiences of countless women who navigate a healthcare system often ill-equipped to recognize and treat the complex symptoms of menopause.
Menopause: A Life Stage, Not a Disease
Menopause is defined as the point at which a woman has gone 12 consecutive months without a menstrual period. It is a natural biological transition, marking the end of reproductive years, rather than a medical condition or disease. The period leading up to menopause, known as perimenopause, can last for several years, characterized by fluctuating hormone levels, primarily estrogen and progesterone, which trigger a wide array of physical, cognitive, and emotional symptoms. Postmenopause refers to the years following menopause.
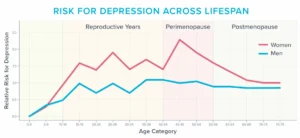
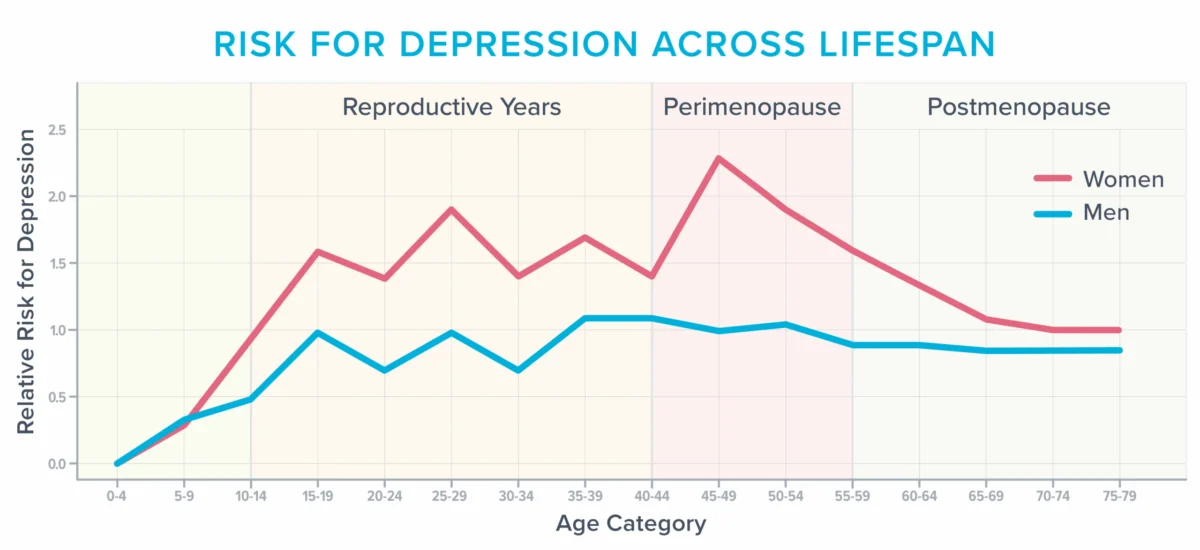
While well-known symptoms like weight gain and reduced libido often receive attention, the impact on mental and emotional health is profound and frequently underestimated. According to the American College of Obstetricians and Gynecologists, approximately 40% of women report increased irritability, mood swings, anxiety, fatigue, and difficulty concentrating during and after menopause. This period also represents one of the most vulnerable times in a woman’s life for developing depression, especially for those with a history of depressive episodes. The accompanying graph illustrates how women’s risk of depression peaks around the perimenopausal years, a stark contrast to men whose risk remains relatively stable throughout adulthood.
Unpacking the Drivers of Cognitive and Emotional Symptoms
The intricate interplay of fluctuating hormone levels, age-related changes in brain structure, and accumulated life stressors contributes to the complex cognitive and emotional landscape of menopause.
- Hormonal Fluctuations: Estrogen, in particular, plays a crucial role in brain health. It influences neurotransmitter production (like serotonin and dopamine), supports neuronal growth, and impacts brain energy metabolism. As estrogen levels decline during menopause, these vital functions can be disrupted, leading to the observed cognitive and mood disturbances.
- Age-Related Brain Changes: While aging naturally brings some cognitive shifts, the hormonal changes of menopause can accelerate or exacerbate these processes.
- Life Stressors: Women in their 40s and 50s often find themselves at the peak of career responsibilities, simultaneously caring for adolescent children and aging parents, managing financial pressures, or navigating significant life changes like an empty nest or marital re-evaluation. These multifaceted demands create a substantial mental load, further depleting cognitive reserves and exacerbating symptoms. A 2022 study published in Menopause journal highlighted that high levels of perceived stress during midlife significantly correlate with increased severity of menopausal symptoms, including brain fog and mood disturbances.
However, a lesser-known but increasingly recognized trigger for cognitive and emotional distress is the vasomotor symptom (VMS)—hot flashes and night sweats.
The Anatomy and Impact of Vasomotor Symptoms

Vasomotor symptoms, characterized by sudden sensations of intense heat, sweating, and often accompanied by heart palpitations, anxiety, and flushing, are more than mere inconveniences. They are a physiological event involving the constriction and dilation of blood vessels, regulated by the hypothalamus, the brain’s thermoregulatory center.
During a hot flash or night sweat, there’s a surge in norepinephrine and cortisol, stress hormones that can further disrupt physiological balance. Blood vessels dilate to shed heat, leading to a temporary increase in heart rate and blood pressure. The prevailing theory suggests that falling estrogen levels affect the hypothalamus, causing it to misinterpret normal body temperature, triggering these intense heat dissipation responses.
For many years, VMS were dismissed as transient, embarrassing symptoms. However, a growing body of research now reveals their significant impact on vascular health and brain function, leading an increasing number of experts to classify them as a treatable medical condition.
VMS and Brain Health: A Deeper Dive
Studies have uncovered concerning links between frequent hot flashes and adverse brain changes:
- White Matter Intensities (WMIs): Research involving women monitored for hot flashes and subjected to MRI scans revealed a correlation between frequent hot flashes and an abundance of whole-brain white matter intensities. These patchy areas, once thought to be a benign consequence of aging, are now recognized as predictive markers for future cognitive decline. Individuals with numerous WMIs are twice as likely to be diagnosed with dementia and three times as likely to experience a future stroke. This suggests a direct pathological link between VMS and microvascular changes in the brain.
- Vascular Health: A three-year study of 492 women demonstrated that those experiencing frequent hot flashes also exhibited unhealthy changes in their blood vessels, such as reduced ability to dilate in response to increased blood flow. This impaired vascular reactivity can compromise blood supply to the brain, contributing to cognitive issues. Other research has linked frequent hot flashes with increased markers of cardiovascular risk, including higher blood pressure, increased arterial stiffness, and elevated levels of inflammatory markers. These vascular changes are particularly concerning given that vascular health is intimately linked to brain health.
- Sleep Disturbances: Frequent hot flashes, particularly night sweats, profoundly disrupt sleep architecture. Many women may not even realize that VMS are the cause of their nocturnal awakenings, attributing them to general insomnia or sleep apnea. The surge of cortisol and norepinephrine can jolt a woman awake, and by the time she registers consciousness, the feeling of heat may have dissipated, leaving her to wonder why she’s repeatedly waking for no apparent reason.
Chronic sleep deprivation, a common consequence of VMS, has a devastating impact on the brain. It impairs the brain’s ability to consolidate memories, process information, and clear metabolic waste products through the glymphatic system. It also leads to reduced connectivity in the hippocampus, a critical region for learning and memory. Furthermore, insufficient sleep makes the amygdala, the brain’s emotion center, hyper-reactive, contributing to heightened stress, anxiety, irritability, and even rage. These changes can manifest within days of poor sleep and accumulate over years, leading to the profound cognitive and emotional deficits experienced by many menopausal women.
Barriers to Effective Care: Why Help is Hard to Find
Despite the clear physiological links, many women struggle to receive accurate diagnoses and appropriate treatment for menopause-related symptoms. Several systemic issues contribute to this problem:
- Diagnostic Overlap with Depression: Standard diagnostic tools like the Patient Health Questionnaire (PHQ-9) depression scale include symptoms like sleep disturbance, fatigue, low energy, and difficulty concentrating—all of which are common in menopause. This overlap means women can easily be diagnosed with depression based on these symptoms, even when the underlying cause is hormonal. A 2017 study in the Journal of Women’s Health found that a significant percentage of women presenting with depressive symptoms in midlife were actually experiencing perimenopausal symptoms that resolved with hormone therapy.
- Lack of Menopause-Specific Medical Training: A major impediment is the pervasive lack of adequate menopause education in medical curricula. Surveys indicate that up to 80% of medical residents feel "barely comfortable" discussing menopause, and few residency programs, including obstetrics and gynecology, offer comprehensive training in this area. This educational gap means many healthcare professionals lack the knowledge to recognize menopausal symptoms beyond hot flashes or to counsel patients on treatment options effectively.
- "Defensive Medicine" and Misinformation about MHT: Even when VMS are identified, many healthcare professionals hesitate to prescribe Menopausal Hormone Therapy (MHT), also known as Hormone Replacement Therapy (HRT). This reluctance often stems from historical concerns rooted in the early 2000s Women’s Health Initiative (WHI) study. While the WHI study initially raised alarms about increased risks of breast cancer, heart disease, and stroke with MHT, subsequent re-analyses and more recent research have provided a more nuanced understanding.
Today, medical societies like the North American Menopause Society (NAMS) and the American College of Obstetricians and Gynecologists (ACOG) largely agree that for women under 60 or within 10 years of menopause onset, and who experience moderate to severe symptoms, the benefits of MHT often outweigh the risks. These benefits include symptom relief, reduced risk of osteoporosis, and potentially a reduced risk of Alzheimer’s disease. The risks are often dose-dependent, hormone-type dependent, and duration-dependent. However, a culture of "defensive medicine," as coined by Michigan-based menopause-trained gynecologist Dr. Jerrold H. Weinberg, persists, where clinicians prioritize avoiding potential litigation over providing optimal care based on current evidence. Antidepressants, while potentially helpful for mood symptoms, do not address the underlying hormonal deficiency and may come with their own side effects, yet are often seen as a "safer" choice by practitioners practicing defensively.
Empowering Advocacy: Navigating the Healthcare System
Given these challenges, women must become proactive advocates for their health. Dr. Weinberg and Helen Kollias, PhD, a science advisor at Precision Nutrition, offer critical advice:
- Seek Menopause-Trained Professionals: Prioritize healthcare providers who list "menopause" as an area of focus or hold certification from reputable organizations like The Menopause Society (formerly NAMS). These professionals are more likely to be up-to-date on current research and treatment guidelines.
- Document Symptoms Meticulously: Maintain a detailed symptom diary. Track the frequency, severity, and triggers of hot flashes, night sweats, brain fog episodes, mood changes, and sleep patterns. Specific data, such as "waking five times a night, with the longest stretch of sleep being three hours," is far more impactful than a vague "I don’t sleep well." Utilize smartwatches or sleep trackers to gather objective data.
- Engage in Shared Decision-Making: Be prepared to discuss the pros and cons of various treatment options with your provider. Ask specific questions about the benefits and risks of MHT for your individual health profile, considering your age, symptom severity, and medical history. This collaborative approach encourages a more patient-centered discussion and can help shift a clinician away from a purely defensive mindset.
Questions to consider include: "What are the specific risks and benefits of MHT for someone with my health history and symptoms?" "Are there different types or doses of hormones that might be more appropriate?" "What are the long-term implications of not treating these symptoms?"
Lifestyle Strategies for Mental and Emotional Health in Menopause
Beyond medical interventions, lifestyle habits play a crucial role in managing menopausal symptoms and enhancing overall well-being.
- Lean into Fundamental Health Strategies: The core pillars of health—nutrition, physical activity, stress management, sleep hygiene, social connectedness, and a sense of purpose—become even more critical during this transitional phase. Regularly assess if you are consistently prioritizing these fundamentals.
- Nutrition: Focus on a balanced diet rich in whole foods, vegetables, fruits, lean proteins, and healthy fats. The Mediterranean and MIND diets, known for their neuroprotective benefits, are excellent models.
- Physical Activity: Engage in a mix of cardiovascular and strength training exercises.
- Stress Management: Incorporate practices like mindfulness, meditation, or yoga.
- Sleep: Prioritize a consistent sleep schedule and optimize your sleep environment.
- Social Connection & Purpose: Maintain strong social ties and engage in activities that bring meaning and joy.
- Experiment with Creatine: Beyond its role in muscle and bone health, creatine (5-7g daily of monohydrate) has shown promise in bolstering mood, improving brain function, reducing mental fatigue, and counteracting some negative effects of sleep deprivation.
- Optimize Light Exposure: Daily exposure to natural light, especially in the morning and late afternoon, helps regulate the body’s circadian rhythm, promoting alertness during the day and better sleep at night. Studies show morning sunlight exposure correlates with quicker sleep onset, longer sleep duration, and fewer awakenings.
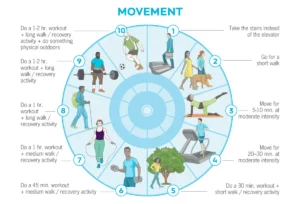
- Mindful Exercise Intensity: While regular physical activity is vital, intense, long-duration workouts can be counterproductive during menopause, especially with sleep deprivation. Recovery takes longer, and injuries are more common. Instead, integrate short bursts of movement (e.g., a 5-10 minute walk or quick squats) to boost alertness, and balance vigorous sessions with moderate activities like Zone 2 cardio or gentle yoga. Listen to your body and adjust intensity based on sleep quality and recovery.
- Investigate Cognitive Behavior Therapy for Insomnia (CBT-I): This evidence-based therapy equips individuals with skills and cognitive reframing techniques to improve sleep. It addresses behavioral patterns and thoughts that interfere with sleep, such as maintaining a consistent wake-up time regardless of sleep quality.
- Get Real About Stress: Evaluate your responsibilities and bandwidth. Identify areas where you can delegate, downsize, or say "no" to free up mental and emotional capacity. The "Wheel of Stress Assessment" can help pinpoint specific stressors. Prioritizing self-care and recovery is not selfish; it’s essential for navigating this demanding life stage.
- Utilize Cooling Technology: A cooler sleep environment can significantly reduce night sweats and improve sleep quality. Experiment with lower thermostat settings, fans, or specialized cooling mattress pads.
- Take Frequent Breaks: When brain fog strikes, productivity plummets. Instead of pushing through, take intentional breaks: step outside, listen to music, stretch, or practice a 5-minute mind-body scan to observe sensations and thoughts without judgment.
- Diet for Healthy Circulation: A diet that supports cardiovascular health also protects brain health. The Mediterranean and MIND diets, rich in vegetables, fruits, whole grains, healthy fats, and lean proteins, are associated with reduced risks of Alzheimer’s disease and depression. Incorporating nitrate-rich foods like beets and dark, leafy greens can temporarily improve memory by enhancing blood flow to the brain.
The Hidden Opportunity of Menopause
While the challenges of menopause can be immense, this life stage also presents a profound opportunity for re-evaluation and personal growth. The limitations imposed by cognitive and emotional symptoms can force a critical assessment of priorities. As one individual reflected, the diminished capacity to "do it all" prompted an existential question: "Do I really need to be doing this?"
This introspection can lead to powerful shifts in how time, energy, and mental resources are allocated. It can empower women to shed unnecessary obligations, simplify daily routines, and prioritize activities that truly matter—nurturing relationships, pursuing passions, and embracing self-care. The journey through menopause, though often arduous, can ultimately lead to a more intentional, balanced, and fulfilling life, transforming a period of struggle into one of profound self-discovery and empowerment.