A significant number of women in their late 40s and early 50s experience profound cognitive and emotional disruptions, often mistakenly diagnosed as depression, when the underlying cause is the hormonal shift of menopause. This misdiagnosis leads to prolonged suffering and inappropriate treatments, obscuring a critical phase in women’s health that demands greater understanding and specialized care. The journey of one individual, initially grappling with severe brain fog, memory lapses, and pervasive fatigue, highlights the systemic challenges in identifying and treating menopause-related symptoms.
The Unseen Struggle: A Personal Account of Cognitive Decline
For nearly two years, a woman in her late 40s and early 50s found herself ensnared in a debilitating mental haze. What began as a frustrating inability to recall proper nouns – a common age-related quirk for many middle-aged individuals – escalated into a pervasive cognitive impairment. Simple tasks like identifying a familiar restaurant, "Texas Roadhouse," became a monumental mental excavation, with details buried under what felt like a "pile of garbage" in her brain. This "sludginess" extended beyond trivial recollections, severely impacting her professional life. She described staring at her computer screen, willing her fingertips to produce constructive work, only to find her mind shrouded in a persistent fog, akin to the groggy moments after silencing an alarm but before full wakefulness. Productivity dwindled to a few fleeting hours of clarity in the mornings, with "worst days" rendering her incapable of work, reading, or any demanding mental activity.
Her quest for answers led her through a revolving door of healthcare professionals. Three doctors recommended antidepressants, which only exacerbated her condition, leaving her feeling "even worse" or "like a zombie." Sleeping pills offered no relief, instead making her feel "more drugged." Extensive tests for thyroid issues and anemia yielded no abnormalities. She experimented with a plethora of supplements, mushroom coffees, and "think"-labeled products, all to no avail. The breakthrough came almost by chance during a routine gynecological exam. A casual mention of vaginal dryness prompted her gynecologist to inquire about a broader range of symptoms: sleep quality, mood, energy levels, hot flashes, and, crucially, brain fog. Her admission of feeling "barely alive" in a "hazy monotone" finally led to the correct diagnosis: menopause. Prescriptions for estradiol and progesterone brought almost immediate relief, as if "someone had flipped a switch," restoring her ability to think, write, converse, and, significantly, sleep more than two hours uninterrupted for the first time in years.
Menopause: More Than Just Hot Flashes
Menopause is not a disease but a natural biological transition, a life stage defined by 12 consecutive months without a menstrual period. This transition, preceded by perimenopause, involves significant fluctuations and a subsequent decline in hormone levels, primarily estrogen and progesterone. While symptoms like hot flashes, night sweats, weight gain, and reduced libido are widely recognized, a less discussed but equally impactful array of symptoms includes increased irritability, mood swings, anxiety, fatigue, and profound trouble concentrating. The American College of Obstetricians and Gynecologists reports that approximately 40 percent of women experience these cognitive and emotional disturbances during and after menopause.
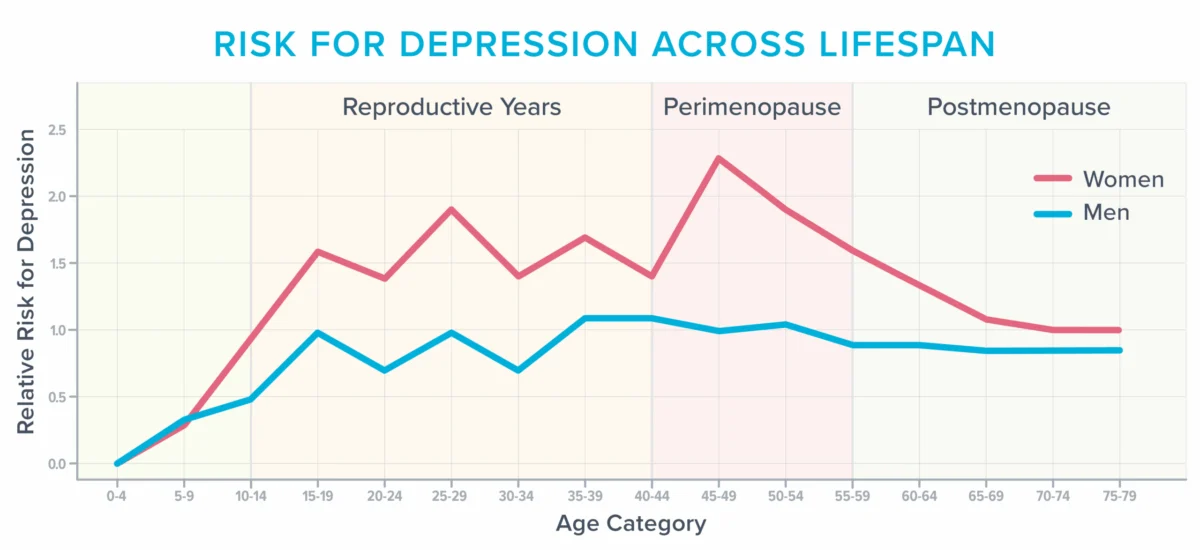
Compounding this, research indicates that the perimenopausal years represent one of the most vulnerable periods for women to develop depression, particularly for those with a prior history of mood disorders. This heightened risk, visually depicted in demographic data showing women’s depression risk peaking around this life stage, underscores the critical need for accurate diagnosis and tailored support. The emotional toll can be immense, as evidenced by experiences of unprovoked sobbing, heightened sensitivity to everyday stimuli, and new anxieties about previously benign situations. These emotional and cognitive shifts can profoundly disrupt daily life, relationships, and professional performance.
The Science Behind the "Fog": Vasomotor Symptoms and Brain Health
The exact mechanisms driving these cognitive and emotional symptoms are complex, involving both fluctuating hormone levels and typical age-related brain changes. Estrogen, in particular, plays a crucial role in various brain functions, including memory, mood regulation, and temperature control. As estrogen levels decline, the hypothalamus, the brain’s internal thermostat, can become dysregulated, leading to the erratic temperature shifts characteristic of hot flashes and night sweats, collectively known as vasomotor symptoms (VMS).
For years, VMS were largely dismissed as mere inconveniences. However, an accumulating body of research now reveals that they are far more significant, potentially impacting brain health and the vascular system. During a hot flash, there’s a surge in norepinephrine and cortisol, leading to blood vessel dilation, increased heart rate, and elevated blood pressure. This physiological stress response is not benign. Studies have linked frequent hot flashes to adverse changes in the brain and blood vessels. For instance, a study involving 226 women found that those experiencing the most hot flashes exhibited a higher prevalence of "whole-brain white matter intensities" on MRI scans. These lesions, once considered benign age-related changes, are now understood to be predictive of future cognitive decline, doubling the risk of dementia and tripling the likelihood of a future stroke.
This vascular connection is further supported by a three-year study of 492 women, which demonstrated that frequent hot flashes correlated with unhealthy changes in blood vessels, specifically a reduced ability to dilate and accommodate increased blood flow. Beyond structural changes, VMS are also associated with increases in inflammation, oxidative stress, and impaired endothelial function—all factors detrimental to cardiovascular and brain health. These findings have led a growing number of experts to reclassify VMS as a treatable medical condition, rather than simply a nuisance.
Beyond direct physiological impact, VMS indirectly affect the brain by severely disrupting sleep. Many women, unaware of the nocturnal hot flashes, attribute their awakenings to insomnia or sleep apnea. The cortisol and norepinephrine surges can jolt them awake, even if the sensation of heat dissipates quickly, leading to frequent, unexplained awakenings throughout the night. Chronic sleep deprivation, even over short periods, significantly impairs the brain’s ability to consolidate memories, metabolize toxins, and store new information. It can also lead to reduced connectivity in the hippocampus, a vital region for learning and memory, and increase the reactivity of the amygdala, the brain’s emotional center, leading to heightened stress, anxiety, irritability, and rage. The cumulative effect of years of such sleep disruption can have profound and lasting consequences on cognitive and emotional well-being.

Navigating the Healthcare Labyrinth: Challenges in Diagnosis and Treatment
The misdiagnosis of menopause-related cognitive and emotional symptoms as depression is a widespread issue, partly due to the overlap in symptom presentation. Standard diagnostic tools like the Patient Health Questionnaire (PHQ-9) depression scale include symptoms such as trouble sleeping, fatigue, changes in appetite, and difficulty concentrating – all of which are common in menopause-related sleep deprivation. A woman experiencing these four symptoms could be diagnosed with depression, diverting attention from the underlying hormonal cause.
A significant contributing factor to this diagnostic gap is the pervasive lack of menopause-specific training within the medical community. Surveys reveal that 80 percent of medical residents feel "barely comfortable" discussing menopause, and few residency programs, including those for obstetrics and gynecology, offer comprehensive training in this area. This deficiency means that many healthcare professionals do not routinely inquire about hot flashes or sleep disturbances when patients present with fatigue, lack of motivation, and cognitive difficulties.
Furthermore, even when VMS are clearly linked to cognitive and emotional symptoms, many healthcare professionals remain hesitant to prescribe menopausal hormone therapy (MHT), often citing concerns about safety and risk. This reluctance, described by Michigan-based menopause-trained gynecologist Dr. Jerrold H. Weinberg as "defensive medicine," stems from a fear of litigation. These fears are largely rooted in older research, particularly studies from several decades ago, which linked certain types of hormones to a slightly increased risk of breast cancer or stroke.
However, more recent and nuanced research has refined our understanding. Current medical consensus indicates that the small increased risks associated with MHT depend on factors such as age, dose, type of hormonal preparation, and duration of use. For women under 60 and fewer than 10 years postmenopausal, particularly those with moderate to severe menopausal symptoms, many experts now agree that the benefits of MHT often outweigh the risks. These benefits extend beyond symptom relief to include a reduced risk of Alzheimer’s disease and osteoporosis. Dr. Weinberg emphasizes that for most women, the health benefits of MHT significantly outweigh the risks. Despite this updated evidence, some practitioners opt for antidepressants to address mood, sleep, and hot flashes, viewing them as a "safer bet" due to defensive medical practices, even though antidepressants carry their own spectrum of side effects.
Empowering Women: Advocacy and Lifestyle Strategies
For women navigating the complexities of menopause and seeking appropriate care, active self-advocacy is crucial. Experts like Dr. Weinberg and Helen Kollias, PhD, a physiology and molecular biology expert, offer practical guidance:
- Seek Menopause-Trained Professionals: Prioritize healthcare providers who explicitly list menopause as an area of focus or who hold certifications from organizations like the Menopause Society. Databases provided by such societies can aid in locating these specialists.
- Document Symptoms Meticulously: Keep a detailed log of symptoms, including their frequency, intensity, and impact on daily life. Specificity is key; instead of saying "I don’t sleep well," note "I wake, on average, five times a night, with my longest stretch of sleep being three hours." This objective data empowers patients during appointments, especially when brain fog may impair recall, and helps track treatment efficacy. Track hot flashes (frequency, severity, triggers), sleep patterns (duration, awakenings, quality), mood changes (irritability, anxiety, sadness), and cognitive function (memory lapses, concentration issues).
- Engage in Shared Decision-Making: Advocate for open discussions about treatment options, including their benefits and risks. Shared decision-making, where clinicians and patients collaboratively make choices based on comprehensive information, can help shift practitioners away from a defensive mindset and ensure care aligns with individual values and preferences. Questions such as "What are the specific benefits and risks of this treatment for me?" and "What are the alternatives, and how do their benefits and risks compare?" are vital.
Beyond medical intervention, a holistic approach incorporating lifestyle strategies can significantly mitigate menopause-related cognitive and emotional challenges:
- Lean into Fundamental Health Strategies: Core healthy behaviors – nutrition, physical activity, stress management, adequate sleep, social connectedness, and a sense of purpose – become even more critical during menopause. Regularly assess and optimize these areas.
- Experiment with Creatine: Beyond its known benefits for muscle and bone health, creatine (5-7g daily of monohydrate) may bolster mood, enhance brain function, reduce mental fatigue, and counteract some negative effects of sleep deprivation.
- Regular Light Exposure: Morning and late afternoon sunlight exposure helps regulate the body’s circadian rhythm, promoting alertness during the day and better sleep at night. It can also positively influence mood and concentration.
- Modify Exercise Routines: Intense, prolonged exercise can exacerbate fatigue and increase injury risk in midlife. Instead, focus on shorter, moderate sessions. Incorporate brief movement breaks (5-10 minute walks, quick sets of squats) to boost alertness. Gentle exercises like yoga or stretching can aid relaxation before bed, but avoid intensity that triggers adrenaline release. Listen to the body, adjusting intensity and volume based on sleep and recovery status.
- Investigate Cognitive Behavioral Therapy for Insomnia (CBT-I): This evidence-based therapy equips individuals with skills and cognitive reframes to improve sleep quality, such as maintaining a consistent wake-up time regardless of prior night’s sleep.
- Get Real About Stress: Menopause often coincides with peak career responsibilities, eldercare, and parenting teens, creating immense cognitive load. Critically evaluate daily responsibilities to identify areas for downsizing or delegating. Tools like the "Wheel of Stress Assessment" can help pinpoint stress sources, facilitating targeted interventions. Learning to say "no" more often can free up mental and emotional bandwidth.
- Experiment with Cooling Technology: A cooler sleep environment can reduce night sweats and improve sleep quality. Options include lowering the thermostat, using fans, or investing in electric cooling mattress pads.
- Take Frequent Breaks: When brain fog sets in, productivity plummets. Instead of pushing through, take intentional breaks (e.g., 20 minutes of quiet contemplation, listening to music, light stretching). A 5-minute mind-body scan can offer a quick refresh, fostering present moment awareness and reducing mental clutter.
- Follow a Circulation-Promoting Diet: Diets rich in vegetables, fruits, whole grains, healthy fats (olives, fish), and legumes, such as the MIND and Mediterranean diets, support both cardiovascular and brain health, reducing risks of Alzheimer’s disease and depression. Nitrate-rich foods like beets and dark leafy greens can temporarily improve memory by promoting blood vessel dilation and increased blood flow to the brain.
Beyond Symptoms: Finding Opportunity in Transition
While the challenges of menopause can be profoundly frustrating, this life stage also presents a unique opportunity for re-evaluation and personal growth. The author’s struggle with diminished cognitive capacity forced an existential reckoning, prompting her to question the necessity of every obligation and how she truly wished to allocate her finite mental resources. This led to a conscious decision to scale back work hours, simplify domestic tasks, and embrace the power of "no," allowing her to prioritize deeply meaningful activities: connecting with aging parents, engaging with her college-aged child, and enjoying leisurely walks with friends.
The eventual relief provided by hormone therapy, coupled with these intentional lifestyle adjustments, restored not only her energy and mental clarity but also a renewed sense of purpose and agency. She continues to conclude her workday earlier than before, not out of necessity, but by choice, demonstrating a powerful shift towards self-prioritization and a more balanced life. Menopause, therefore, can be a catalyst for profound self-discovery, prompting women to redefine their boundaries, reallocate their energy, and embrace a stage of life where well-being takes precedence over relentless productivity.
References
Click here to view the information sources referenced in this article. (Original article’s reference link)